
Forgetting Space
The Architecture of Dementia in Hong Kong
January - May 2019
Selections from Undergraduate Thesis at Cornell University
Semester Project in various medium
Individual Project (Advised by João Almeida & Timur Dogan)
I selected pieces that described the research, design and thinking process of this project. This project is my attempt to start a conversation about patient advocacy in the built environment, especially with increasing aging population rooted in a city where the physical topographical and infrastructure presents many obstacles.
Overview
“I want to go home” - this is a harrowing cry of many patients with Alzheimer’s disease everyday, usually during sunset. Grandpa called the home number with this request - we passed the phone around to mom, to our helper Lina, then to me. We never really knew what to say. We went through a round a stories aimed to distract him. We felt guilty for supplying these narratives. We didn’t want to lie to him. We also knew that he would forget these narratives - his forgetting would somehow invalidate some of these stories aimed to distract. It was very frustrating for caregivers and family members, because the patient is physically already home but he/she is thinking of a home from many years in the past. This very scenario is brimming with questions surrounding the reliability of memory, projections of the recreated past, and what it means to live in the immediate sensorial. The conflation of time, memory and space inspired this project. The disease speaks to the fear of losing yourself, the fear of forgetting precious memories and the fear forgetting how to function. One is slowly relinquishing his/her autonomy over the course of the disease - from the innocuous act of misplacing keys, to repeating things in conversations to even forgetting how to swallow food.
I am responding to the condition with an attitude of palliative care and acceptance, especially when Alzheimer’s Disease has no cure. No, designed spaces cannot relieve the pain that your loved one might forget who you are, but, it can potentially create the conditions for more good days, and higher quality immediate experiences for the patient in real time. This thesis proposes a new typology of domestic architecture in Hong Kong. The design of the prototype is rooted in the ritualistic and sensorial daily habits of bathing, eating and sleeping. These cyclical experiences between the caregiver and the patient are then framed in different socio-anthropological hierarchies of the city. How much does one remember in a space? What role does exaggeration, illusion and preference warp one’s perception of space? The bridge between the ephemeral state of memory and the practical concerns of accessibility might possibly revive the patient with a version of previously lost independence and autonomy.
I had the privilege of presenting the project to Gensler’s Inclusivity Network (GIN) - the call was attended by over 50 people firm wide. As a result of the call, I was recommended to the product design department and pitched several proprietary product developments in bathroom, carpet and tiling accessories for Alzheimer’s patients.
Although the thesis itself, and the results of the product development pitches were both inconclusive, I am still fascinated with the implications of the project and I hope to continue this interest at the RCA as well as in professional practice. I care deeply about inclusive design and designing for the aging community, especially in the role that the built environment plays to support and empower. I have furthered my interest through attending online courses in gerontology and inclusive design | Fundamentals of Gerontology, University of Southern California, Leonard Davis School of Gerontology and the American Society on Aging, September - October 2020. An Introduction to Accessible and Inclusive Design, University of Illinois at Urbana Champaign, September – October 2020. Disability Awareness and Support, University of Pittsburgh, July - August 2020.
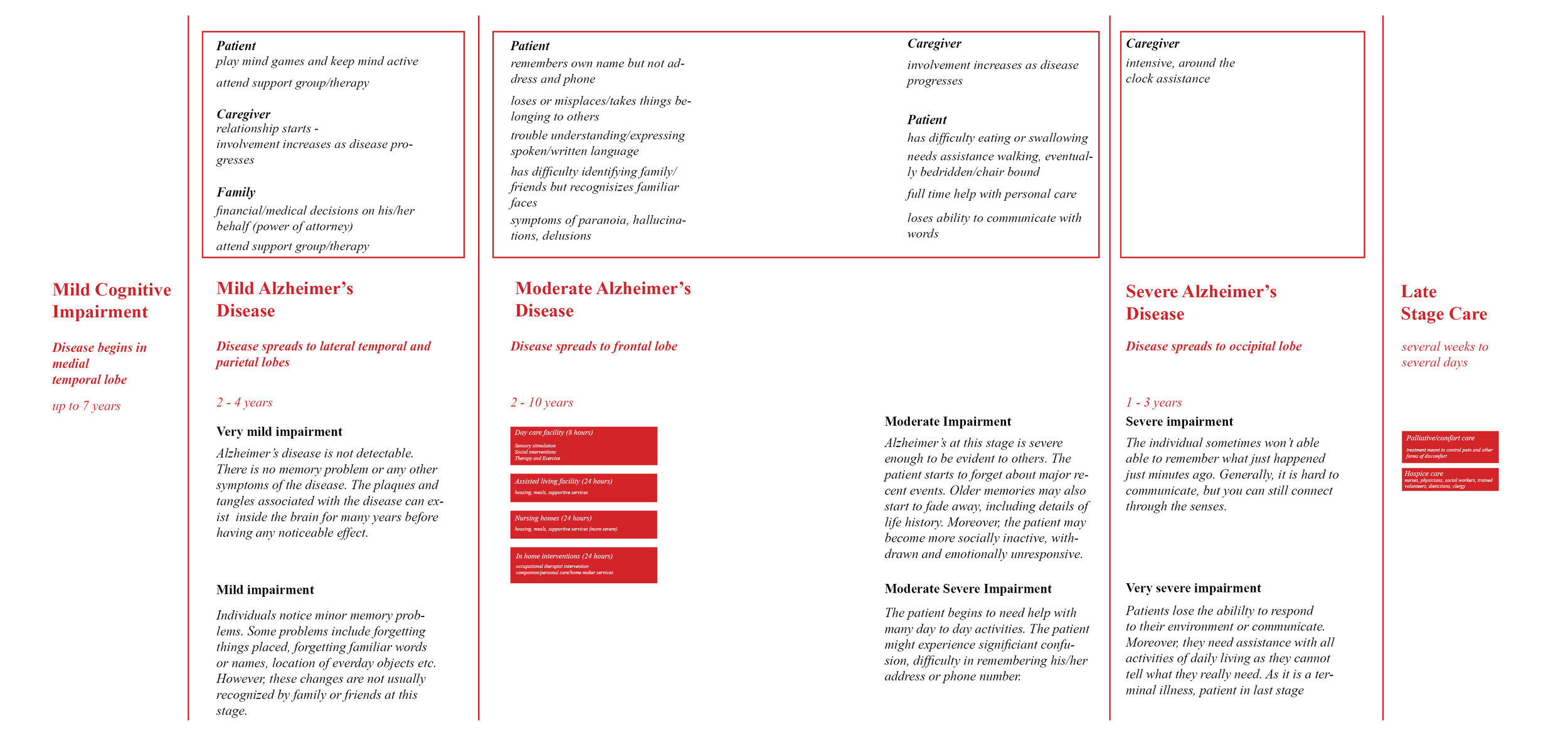
Catalogue of Changes

I started the project by documenting rituals in daily life that might become irritating, distressing or even dangerous for Alzheimer’s patients. The scenarios for these drawings are a result of what I learned from volunteering at the Hong Kong Jockey Club Centre for Positive Ageing, interviews with caregivers as well as the book, “Lost in Space: Architecture and Dementia”, Feddersen, Eckhard, Insa Lüdtke, and Julian Reisenberger.
Through this exercise, it became clear that there are seemingly innocuous design elements that cause distress. Some symptoms of Alzheimer’s Disease have performative and spatial implications. The most characteristic feature of the disease is the patient’s lack of short term memory. This alone suggests the experiential phenomena of an ephemeral architecture of immediate consumption.

Hong Kong is a city without ground. It struggles to grapple with its cultural roots through deliberate cycles of historical erasure. Its steep topological condition and dense stacking or residential, commercial and transportation infrastructure obliterates figure-ground in the city, and in-turn redefines public-private spatial relationships. With a sharply increasing aging population, there is still a lack of subsidised elderly facilities that have specialized services catering to dementia sufferers.

Sundowning or Sunset Syndrome is used to describe the big changes in how dementia patients act during during the late afternoon or early evening. It can cause a variety of behaviours, such as confusion, anxiety, aggression and lead to pacing/wandering. There are architectural implications of this behavioural trait. It implies an architecture that shields light at certain times, a schedule that distracts the patient, a schedule that brings the patient away from natural light during sunset.

Wandering and getting lost is common among people with dementia and can happen during any stage of the disease. The patient may not remember his or her address, sense of direction, and purpose of the walk. Additionally, diminishing motor skills increase the risk of the patient slipping/falling.

Habits such as, swallowing medication, forgetting the differences between hot and cold water, how to wear shifts, seeing the toilet and aiming, locating the remote, oversleeping, forgetting to turn off the tap and slipping in the bathtub occur everyday. Are their architectural solutions to makes these daily rituals easier?

Repeating questions could become frustrating for the caregiver/family. The repetition is often due to stress, anxiety or frustration. Due to the patient being unsure of what is happening, where he/she is, the patient may feel very frustrated and confused. This characteristic is frustrating for both the patient and the caregiver. An architectural intervention that provides both a sense of safety/stability, yet provides the conditions for new questions might be a solution to this.

Patients find it increasingly difficult to differentiate between similar colors. The best example is a white toilet seat cover, on a white toilet bowl on white bathroom tiles. By changing the seat cover to a color like red, it is much easier for the patient to see and aim.

Some patients mistake windows as cabinets or drawers. This causes the unfortunate, unintentional incident of shoes falling from the sky. There is a universality in the way patients understand and react to architectural elements at all stages of the disease. Patients may experience confusion when in a corridor, but when faced with a door, patients will always walk towards it. When faced with a window, patients will always look towards it and even walk towards it. Such spatial and object misreadings have a lot of design/generative potential.As a response, windows that have “nets” or windows are are slightly recessed provide a buffer for the object to fall on. It is a preventative design move.

Patients sometimes forget their own reflection. Mirrored and shiny surfaces may stimulate the senses too much and cause distress. Many patients also talk to their own reflection for many hours. However, some become irritated when he/she realizes that “the other person” would mimic his/her every move.

Morphology of Architectural Elements | Morphology of the Door I learned that doors cue movement: Dutch doors/Stable Doors provide a sense of security and openess while delineating the spaces and boundaries between two rooms. The proportion of the cut, relative to the human body provides that sense of comfort. They are mainly used in Alzheimer’s units in case a patient misbehaves. Double Doors with a slight gap gives the caregiver a chance to peek into the space. The lack of window on the door and lack of door knob on the patient’s side of the room does not incite any desire for the patient to see the “door” and want to leave. The Revolving Door restricts entry and exit to one person at a time. It is ideal for providing security in old folk’s home in case someone decides to wander. The door slows down circulation to create the conditions for surveillance. The glass windows on doors make it easy for nurses and doctors to glance into the ward quickly. The porous door creates the ideal conditions for surveillance.
Site Research
I was developing the catalogue and simultaneously exploring site options. I initially envisioned this project to be a series of interventions that vary in scale and scope, peppered throughout Hong Kong. I started by photographing different parts of the city – I focused on spaces that are fast and slow, singular and repetitive, dense and sparse. I felt that these co-existing dualities was what made Hong Kong different and especially challenging to patients with Dementia.
Hong Kong is a city without ground. It struggles to grapple with its cultural roots through deliberate cycles of historical erasure. Its steep topological condition and dense stacking of residential, commercial and transportation infrastructure obliterates figure-ground in the city, and in turn redefines public-private spatial relationships. Perception of distance and time is distorted through compact networks of pedestrian infrastructure, public transport, and natural topography in the urban landscape. With a sharply increasing aging population, there is still a lack of subsidized elderly care facilities that had specialized services catering to dementia sufferers.
After presenting the series of photographs, I narrowed my options and decided on four sites: the inside of a moving tram, an abandoned health center in Shek O, a closed theatre in North Point, and the Happy Valley Racecourse. These were all locations that carried historic significance during the 1940-60s. They also carried implications of something cyclical, performance-like, tactile and sensorial. Additionally, these sites presented physical challenges of access and mobility.
However, as a result of the first review where I presented these images and parts of the developing catalogue, we decided that it would be helpful to narrow the scope and focus the project on daily habits and rituals. I agreed with the critics and decided to follow their advice. I am still happy with the photographic explorations of this part of the project, and I wanted to include them as part of my RCA portfolio to showcase my creative process.





















Learning from De Hogeweyk
Routine, observation & surveillance: Truman Show/Dementia Village
De Hogeweyk is a nursing home disguised as a functioning neighborhood. It is equipped with curated supermarkets, restaurants, hair salons etc. to create conditions for the residents to be challenged by recognizable incentives to remain active in daily life. Although patients cannot leave the facility, they are able to roam freely within its confines. The interior of the village is structured by a series of small outdoor courtyards, green areas, gardens and central boulevard. The main entrance serves a security gate to ensure that staff can intercept residents that try to leave. Hogeweyk can be interpreted as a type of 24 hour surveilled Truman Show purgatory designed to fabricate aspects of each individual’s sense of what is familiar. The premise of the village challenges the notion of what constitutes private and public space. This constructed utopia can be scrutinized as a dystopic pleasure prison.

Daily Schedule
A comparison between De hogeweyk & Bellevue Heights | Familiarity & Routine as Anchor Points
I was noticing similarities between the planned activities between the patients at De Hogeweyk and patients at the Hong Kong Center for Positive Aging. Since De Hogeweyk is designed and staged more like a private residence, I wanted to map and compare routines and timestamps between De Hogeweyk and my grandfather’s routines with his caregiver. I was able to conduct movement surveys by tracking my grandfather’s movements during the day. I spent 2 weeks living with him and grew familiar with his routine. His routine is deliberately regimented and strict: the familiarity creates the conditions for comfort.
Caregivers and patient have a dialectic relationship. Caregivers curate, design and manage the patient’s routine. The actions in the routine control the patient’s health and wellbeing. They are in charge of the patient’s hygiene, feeding, mobilisation and exercise and the client’s emotional and social well being. When the patient falls asleep, this is a signal to the caregiver. The routine is so ingrained that the caregiver knows exactly when the patient goes to the bathroom. The patient doesn’t know this and memory resets. There is an asymmetric relationship of surveillance.
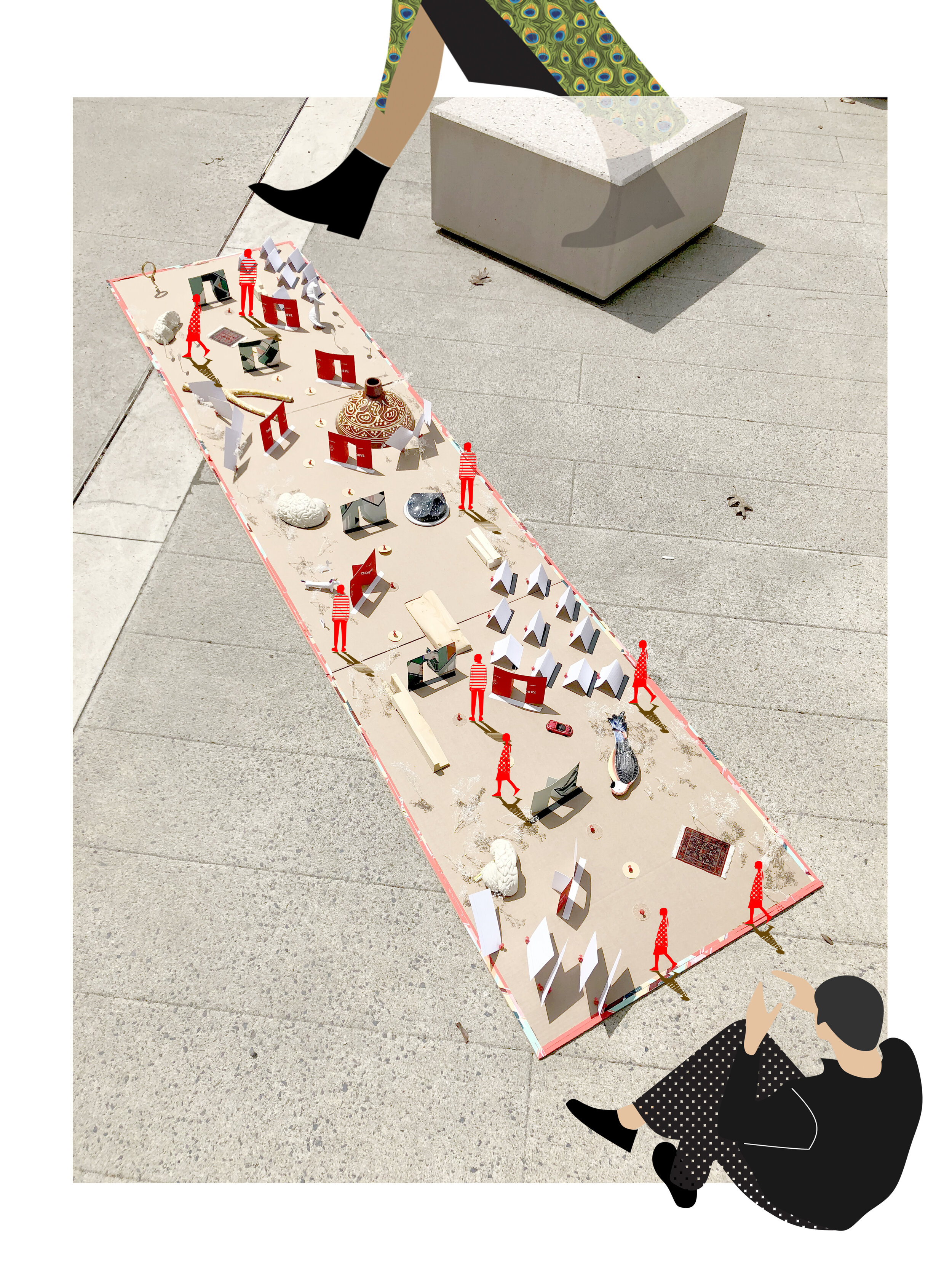
Design Based on Routines
The routines anchor the person, but the walls move and collapse inward according to the shifting needs of the patient as the disease progresses. This is the rationale and design I proposed as a topic of discussion. Practicality and existing technology aside, this is an interesting proposal for patients in Hong Kong.







Case Studies
As a result of what I learned from the spatial mapping exercises and catalogue, I decided on focus on the caregiver v. patient dynamic as it relates to culture and policy in Hong Kong. The caregiver’s patience and mood is directly correlated with the patient’s health. However, the symptoms of the patient, for example, the habits of repeating stories, questions and simple tasks, the patient’s crying, could be very draining for the caregiver, especially considering the length of the disease.
I thus created a series of apartment case studies that create the conditions for more patient, caregiver interaction and opportunities for communication. Perhaps as a chance to reduce the caregiver’s stress. This is a direct response to the problematic global malpractice of caregivers unnecessarily prescribing patients with sedatives and antipsychotic drugs as an easy, short term pacifiers for behaviors that are “annoying nuisances” that only further reduce that patient’s autonomy. They are designed to create the conditions that create less opportunity for patient irritability. They also address the patient’s increased clumsiness.
As a result, this new catalogue of spaces challenge the hierarchy between the servant and the served. The bridge between the ephemeral state of memory and the practical concerns of accessibility might possibly revive the patient with a version of previously lost independence and autonomy. The rich plethora of spatial conditions, with the patient and caregiver forgetting the default positions acts as a social hierarchical equalizer.
The spatial proportions and distributions of rooms are informed the tectonic language of precast concrete apartment blocks of Hong Kong during the 1970s. The efficient form corresponds to the housing boom of 1973, as a direct result of 400 percent population increase baby boom post WW2. Conceptually, this spatial/tectonic consistency adds a degree of familiarity for this generation of patients.
The project scale is also deliberately introspective and within the private apartment scale. I am responding to the strongly held cultural pressures of filial piety which assumes that the care of the elderly will be provided primarily, perhaps exclusively caregivers, from members of the family or employed caregivers. There also seems to be a lot of guilt surrounding family members that feel that they are abandoning their loved ones by placing them in a nursing home. In Hong Kong, there are many cognitive, and cultural anthropometric implications of the “caregiver”.

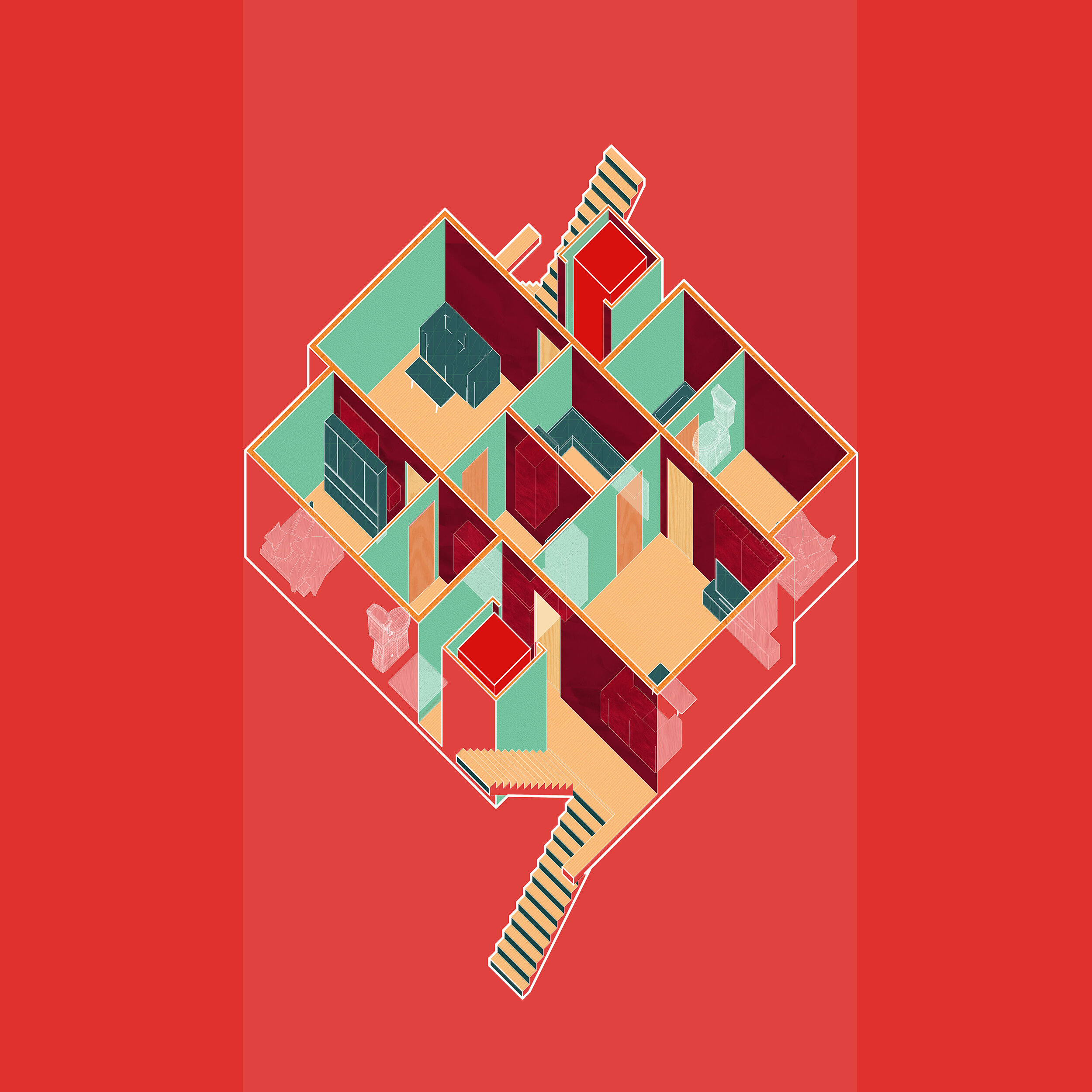
Scenarios
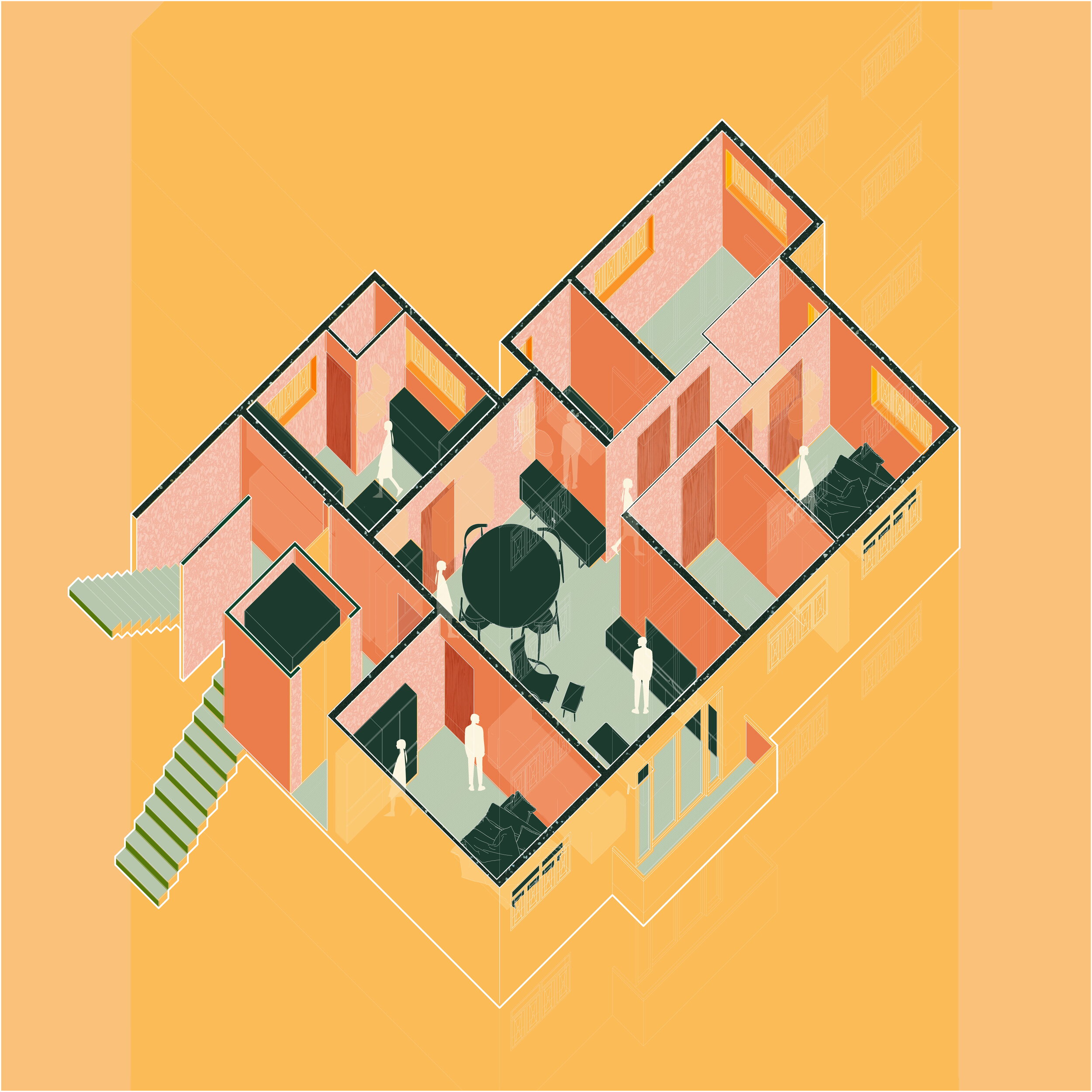
Default | Typical 1970’s Hong Kong Apartment | This was the benchmark plan for the basis of design. In existing building plans, how can days be programmed to stimulate the patient’s senses and create conditions for good days.

Act 2 | Caregiver as Foreign Domestic Worker | This iteration speaks to the caregiver as a foreign domestic worker that is most often Indonesian, Filipino or Sri Lankan. They live under the government’s stipulated live in law of 2003, for “full time live in domestic service”.
Act 3 | Caregiver from the Mainland/Local | This iteration speaks to the increasing popularity of caregivers from Guangdong (mainland China). They do not qualify for the live in law of 2003.

Act 4 | Caregiver as a member of the family | This iteration speaks to filial piety in which a family member lives in with his or her loved one. In Hong Kong, there is a culture of caregiving obligations that Hong Kong Chinese daughters have towards their frail elderly parents.

Act 5 | The Architecture Becomes the Caregiver | This iteration speaks to an architecture that becomes the caregiver. It physically transforms during the course of the patient’s illness.
Act 6 | The Patient becomes his or her own Caregiver | I am responding to the universality of the way patients understand and react to architectural elements at all stages of the disease. The home is treated as a theatre and as game.

The final panel of critics consisted of Joao Almeida, Timur Dogan, Leslie Lok, Anya Bokov, David Leven, Hansy Better Barraza and Peter Christensen.
What I learned from Peter and Hansy’s critique about the role of activism in this project was particularly memorable. I pointed out issues of filial piety and gendered hierarchies that are very present in the patient and caregiver dynamic. However, the schemes that I was proposing to the Hong Kong House Society only amplify existing stereotypes and hierarchies between the caregiver and patient - as Hansy pointed out, I am not liberating the woman. Hansy’s other point about exploring domesticity was also memorable. The design component of this project is undercooked and using the patient’s movement cues as a design strategy was a missed opportunity. I appreciated Leslie’s comment about the extreme breadth of this project. She believes that each strand of the project could have been its individual thesis project. The project could have benefited from more focus and depth.